
We know that consuming enough essential fatty acids is vital to support our health and wellbeing – they are called essential for a reason after all.
However, understanding how to balance these essential fatty acids, as well as to decipher which ones would be most beneficial for our unique health requirements, is where it can get a little bit confusing.
We’ve written extensively on the importance of omega-3 fatty acids for health, as well as their broad role in supporting a plethora of health conditions. But what about omega-6? Is it purely pro-inflammatory or does it also have a place in alleviating inflammation?
In this article, we will explore what essential fatty acids are; the forms and functions of omega-3 and omega-6 fatty acids, as well as the latest research on the uses of GLA, and the combined role of EPA, DHA and GLA in the body.
What are essential fatty acids?
Essential fatty acids (EFAs) are biologically active fats which the body requires to support several important functions from blood clotting to inflammation; differentiating them from other fats which are either stored or used for energy. EFAs are deemed ‘essential’ because humans and other animals cannot produce them; meaning that they must be consumed from food.
The two types of fatty acids which are essential to the body are omega-3 (ALA) and omega-6 (LA). Other fatty acids such as EPA, DHA and GLA are considered ‘conditionally essential’ as they may become essential under certain developmental or disease conditions. While omega-9 is often referred to in association with EFAs, it is not strictly essential as it can be made by the body.
Anthropological evidence suggests that human beings evolved to consume omega-6 and omega-3 fatty acids in a ratio of around 1:1,1 however in the Western world today that ratio is closer to 16:1. While there is no definitive ideal ratio for consumption of these fatty acids, studies suggest that a ratio of between 1:1 and 4:1 is most healthful.2,3
Omega-3
Omega-3 fatty acids are a type of polyunsaturated fat with multiple double bonds, where the first double bond is between the third and fourth carbon atoms from the end of the carbon atom chain. “Short chain” omega-3 fatty acids have a chain of 18 carbon atoms or less, while “long chain” omega-3 fatty acids have a chain of 20 or more. While there are many types of omega-3 fatty acids (differing according to chemical shape and size), the three most common include ALA, EPA, and DHA:
- Alpha-linolenic acid (ALA): as the parent omega-3 fatty acid, it can be converted into EPA and DHA when necessary. However, this process may not be efficient in most individuals, with studies demonstrating that only 8% is converted into EPA and between 0-4% into DHA in healthy young men.4 In healthy young women, this increased to 21% EPA and 9% DHA.5 (The increased conversion capacity in women appears to be related to the effects of oestrogen.6,7)
- Eicosapentaenoic acid (EPA): the primary role of this fatty acid is to create chemical compounds called eicosanoids which play a role in reducing inflammation. EPA has been shown to reduce total cholesterol levels,8 platelet aggregation (clumping)9 and symptoms of depression.10
- Docosahexaenoic acid (DHA): DHA accounts for 40% of the brain’s polyunsaturated fats and is essential for supporting its normal function and development. For years, it has been recommended that pregnant mothers consume DHA to support the optimal growth and development of the foetal brain, while studies have revealed that individuals with Alzheimer’s disease have lower levels of DHA.11
Omega-3 fatty acids are a crucial part of human cell membranes, with several important functions including supporting cognitive12,13 and cardiovascular health,14–16 weight management,17 infant brain development18 and decreasing liver fat.19
In addition to gender differences, genetic variability in enzymes involved in fatty acid metabolism influences one’s ability to generate long-chain polyunsaturated fat (EPA, GLA, DHA and AA).20,21
Omega-6
Omega-6’s ‘pro-inflammatory’ moniker implies that it is not very good for us. While this may be true for some omega-6 fatty acids when taken in excess, it is not the case for all of them. Like omega-3, omega-6 fatty acids are also composed of polyunsaturated fatty acids, but in omega-6 the first double bond in the hydrocarbon chain occurs between the sixth and seventh carbon atoms from the end of the molecule most distant from the carboxylic acid group. There are four types of omega-6 fatty acids: AA, LA, GLA and CLA:
- Linoleic acid (LA): this is the parent omega-6 fatty acid. It is found in nuts, seeds, butter and vegetable oils; and is often consumed in excess in the Western world. While LA can be converted into GLA, when we have an excess of AA in the body, it prevents the conversion of LA into GLA. When this conversion is inhibited, it can cause an imbalance between pro-inflammatory LA and AA, and anti-inflammatory GLA in the body.
- Arachidonic acid (AA): found in meat, eggs and dairy, AA is needed to support muscle growth, brain development and a healthy nervous system. However, we only require very small amounts of this fatty acid and when consumed in excess, it can promote inflammation.
- Gamma-linolenic acid (GLA): found in borage (also known as starflower), evening primrose, echium and hempseed oil, this is a unique omega-6 fatty acid which demonstrates a variety of anti-inflammatory properties. It is essential for supporting brain function, metabolism, bone and reproductive health; as well as stimulating skin and hair growth. The idea that we don’t require GLA due to the high amounts of omega-6 consumed in our diet is a common misconception, when in fact, GLA is vital in order to neutralise and reverse the effects of an excess of AA and LA fatty acids in the diet.
- Conjugated-linoleic acid (CLA): found in animal products such as meat, cheese and butter, as well as white button mushrooms, CLA plays a role in supporting the body’s inflammatory and immune responses, with some studies indicating a role in detoxification by boosting liver function.22,23
Fatty acids, inflammation and prostaglandin creation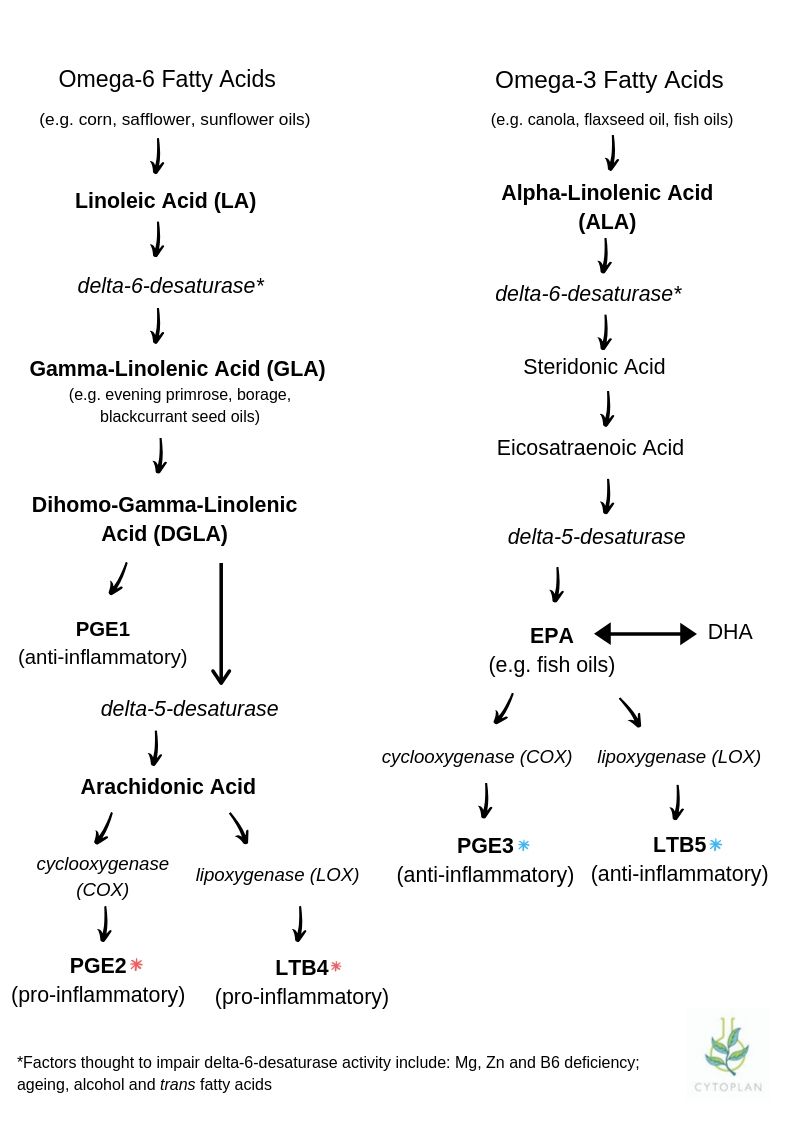
One of the key compounds generated from fatty acids are hormone-like substances called prostaglandins. The primary role of prostaglandins is to support the healing process by balancing inflammatory and anti-inflammatory processes. They are found in almost every cell and tissue throughout the body and are essential to proper functioning.
The three major prostaglandins in the body include PgE1, PgE2 and PgE3:
- PgE1 (anti-inflammatory) – formed from omega-6 fats; either LA or GLA sources
- PgE2 (inflammatory) – primarily derived from AA
- PgE3 (anti-inflammatory) – formed from omega-3 fats; either ALA or more directly from EPA sources
PgE1 is the most potent anti-inflammatory prostaglandin in the body. It is produced through the metabolism of LA into GLA, however this reaction is slow and can be impaired by a variety of factors (see below). Furthermore, proper digestive, liver and enzymatic function are essential for ensuring that the fats consumed in the diet can actually be converted into prostaglandins. It is important to note that both inflammatory and anti-inflammatory prostaglandins are essential, it is only when the system falls out of balance and creates too much PgE2 at the expense of PgE1 and PgE3 that issues arise.
Prostaglandin inhibitors:
- NSAIDs and Aspirin – works by inhibiting PgE2 by blocking the enzyme needed for conversion of the fats. NSAIDs also shut down PgE1 and PgE3 production in the same way and so both inflammatory and anti-inflammatory processes are blocked.
- Alcohol – both PgE1 and PgE3 are inhibited by alcohol, whereas PgE2 is not.
- Sugar – too much insulin in the body causes some of the fats involved in PgE1 formation to be converted into AA, which supports PgE2 formation.
- Trans fats – can inhibit the ability of delta-6-desaturase, the enzyme which converts LA into GLA when consumed in excess.
- Steroids – part of the anti-inflammatory mechanisms of corticosteroids includes the inhibition of prostaglandin synthesis.
- Stress – a decreased synthesis of PgE1 and PgE3, with an increase in PgE2 results in response to higher levels of cortisol in the system.
- Deficiencies – suboptimal levels of magnesium, vitamin B6 and zinc can also inhibit the process responsible for prostaglandin formation.
- Health conditions – evidence suggests that conditions such as hypertension, arthritis, psoriasis and metabolic syndrome may impair the ability of the delta-6-desaturase enzyme.
Omega-3 and omega-6 fatty acids compete for the same conversion enzymes and so consuming a high level of dietary omega-6 may cause issues even in the context of high dietary omega-3.
What does the research have to say about GLA consumption?
GLA has been used for centuries as part of homeopathic remedies, however, it is only in recent years that the research has caught up and several benefits have been confirmed and discovered:
- Anti-inflammatory: GLA is converted into ‘dihomo’ GLA or DGLA and this is incorporated into cell membrane phospholipids. DGLA competes with AA for the COX and LOX enzymes. From the COX DGLA reaction, PgE1 and thromboxane A1 are produced. These compounds exert potent anti-inflammatory, anti-aggregation and vasodilatory actions. 15-HETrE, is produced from the DGLA LOX interaction and inhibits leukotriene B4 production (a pro-inflammatory mediator which stimulates the production of several cytokines to augment and prolong tissue inflammation).24,25 Human studies have revealed that when EPA and DHA are introduced in a balanced ratio to GLA, elevations in serum AA are prevented; leading to a reduction in levels of pro-inflammatory prostaglandin.26,27 (It should be noted that this conversion requires adequate zinc, magnesium and vitamin B6 as cofactors).
- Hormonal balance: PgE2 triggers the inflammation behind uterine contractions which induce the monthly shedding of the uterine lining or menstrual bleeding. When PgE2 is present in excess, cramping can ensue. As a source of PgE1, GLA may be helpful in neutralising levels of PgE2 and supporting pain reduction. In fact, studies have revealed a decreased level of GLA in the system of women suffering from PMS.28 Another area of hormonal balance where GLA is often applied is as menopausal support. While evidence is limited regarding the exact mechanisms, GLA rich evening primrose oil has been found to reduce hot flushes, as well as their frequency and duration.29 In 2018, researchers also discovered a positive reduction in hot flashes, depressive and cognitive symptoms related to menopausal transition following administration of combined EPA, DHA and GLA.30
- Diabetes: studies have shown that supplementing with GLA could reduce symptoms of nerve pain and prevent nerve damage in patients with type 1 or type 2 diabetes.31,32 In fact, it has been observed that a defect in the enzyme which converts dietary fats into GLA may predispose people to develop insulin resistance.33
- Skin health: several studies have shown a positive correlation between improvements in clinical eczema scores and increased intake of EFAs.34 In trials of both children and adults, supplementation with GLA resulted in less inflammation, dryness, scaling and overall severity of eczematic symptoms.35–37
- Allergies: inflammatory eicosanoids (leukotrienes) derived from AA are thought to play a role in the pathology of asthma.38 Daily consumption of combined GLA and EPA improved self-reported asthma status and reduced reliance on inhaler drugs in adults with mild to moderate asthma.39 It is believed that this effect may be due, in part, to GLAs suppression of leukotriene production, a type of inflammatory cytokine which many asthma drugs aim to inhibit.
- Cognitive health: a 20-week RCT revealed that a combined EFA supplement providing 750mg of EPA/DHA and 60mg GLA resulted in improved reading, spelling and non-verbal cognitive development in children aged 3-13.40 A similar study conducted on young adults found that a combination of evening primrose oil (providing GLA) and EPA/DHA resulted in increased cognitive performance and functional brain activation.41
- Heart health: GLA was found to reduce the tendency of platelets to aggregate, or clump together, within small blood vessels,42 which is a vital component in reducing stroke and heart attack risk. It also showed promise for lowering LDL and triglyceride levels, while increasing HDL.43,44 Interestingly, when GLA was combined with EPA and DHA, the heart protective effects appeared even more powerful. Blood pressure was significantly reduced in those with peripheral arterial disease, while a trend toward fewer coronary events was also revealed.45
- Arthritis: several studies have revealed the positive application of GLA in cases of rheumatoid arthritis (RA). In RCT studies, treatment with GLA lowered scores of pain, swollen joints and tenderness.46,47 When immune cells from RA patients were treated with GLA, the production of the inflammatory cytokine IL-1beta was reduced by 40%, without affecting normal immune cell function.48 Suppression of the inflammatory cytokine TNF-alpha was also shown,49 with some research suggesting that DGLA may act directly on T-cells to modulate immune response in diseases such as RA.
- Eye health: studies suggest that a combination of EPA, DHA and GLA may be beneficial for supporting eye health, particularly dry eye. An RCT revealed that combined GLA, EPA and DHA supplementation improved symptoms of ocular irritation, maintained corneal surface smoothness and inhibited conjunctival dendritic cell maturation in patients with postmenopausal keratoconjunctivitis sicca (dryness of the membrane which lines the eye).50
The complementary actions of omega-3 and omega-6
As we can see, there are far-reaching benefits to the inclusion of EFAs in the diet. For some, it may be of extra benefit to consume these fatty acids in their active forms (EPA, DHA and GLA) to avoid competition for conversion enzymes. While often considered individually, it is clear from the research that in many cases, the combined use of these EFAs may be appropriate.
Key Takeaways
- Essential fatty acids, or EFAs, are biologically active fats which cannot be made by the body and are required to support several important functions such as blood clotting and inflammation.
- Omega-6 and omega-3 are being consumed in approximately a 16:1 ratio in the Western world, while between a 1:1 and 4:1 ratio is considered more healthful.
- The three most common omega-3 fats include ALA, EPA and DHA while the four types of omega-6 fatty acids are LA, AA, GLA and CLA.
- One of the key compounds generated through fatty acid consumption are hormone-like substances called prostaglandins whose primary role is to support the healing process by balancing stimulation of inflammation and anti-inflammation processes.
- Factors such as high stress, alcohol use, certain medications and consuming sugar in excess can inhibit the production of anti-inflammatory prostaglandins while encouraging an increase in pro-inflammatory output.
- A combination of EPA, DHA and GLA have been found to support a plethora of conditions such as metabolic syndrome, heart health, asthma, hormonal balance, menstrual pain, skin, cognitive and eye health.
If you have questions regarding the topics that have been raised, or any other health matters, please contact:
nutrition@cytoplan.co.uk, 01684 310099
Relevant Cytoplan Products:
Omega Balance – cold pressed vegan Omega Balance provides 500mg of omega-3 (150mg DHA and 75mg EPA) and 500mg of omega-6 (46mg GLA) per capsule.
Evening Primrose Oil – cold pressed evening primrose oil, providing 500mg of omega-6 (10% GLA) per capsule
Omega-3 Vegan – derived from marine algae – a vegan source of the important omega-3 fatty acids EPA and DHA. Two capsules provide 334mg DHA and 166mg EPA.
Krill Oil – providing 1000mg of krill oil (150mg EPA and 90mg DHA) per two capsules, as well as vitamin A, phospholipids and astaxanthin.
R-Omega – a phospholipid rich DHA and EPA omega-3 supplement from herring roe. Providing 500mg omega-3 (34omg DHA and 100mg EPA) per two capsules, as well as 280mg phosphatidylcholine and 320mg phosphtidylserine.
Fish Oil – high potency fish oil capsules provide 550mg of omega-3 fatty acids (330mg EPA and 220mg DHA) per 1000mg.
References:
- Simopoulos AP. Evolutionary aspects of diet, the omega-6/omega-3 ratio and genetic variation: nutritional implications for chronic diseases. Biomed Pharmacother. 2006;60(9):502-507. doi:10.1016/J.BIOPHA.2006.07.080
- Kris-Etherton P, Taylor DS, Yu-Poth S, et al. Polyunsaturated fatty acids in the food chain in the United States. Am J Clin Nutr. 2000;71(1):179S-188S. doi:10.1093/ajcn/71.1.179S
- Wang S, Wu D, Matthan NR, Lamon-Fava S, Lecker JL, Lichtenstein AH. Reduction in dietary omega-6 polyunsaturated fatty acids: Eicosapentaenoic acid plus docosahexaenoic acid ratio minimizes atherosclerotic lesion formation and inflammatory response in the LDL receptor null mouse. Atherosclerosis. 2009;204(1):147-155. doi:10.1016/j.atherosclerosis.2008.08.024
- Burdge GC, Jones AE, Wootton SA. Eicosapentaenoic and docosapentaenoic acids are the principal products of α-linolenic acid metabolism in young men. Br J Nutr. 2002;88(4):355-363. doi:10.1079/BJN2002662
- Burdge GC, Wootton SA. Conversion of α-linolenic acid to eicosapentaenoic, docosapentaenoic and docosahexaenoic acids in young women. Br J Nutr. 2002;88(4):411-420. doi:10.1079/BJN2002689
- Burdge G. Alpha-linolenic acid metabolism in men and women: nutritional and biological implications. Curr Opin Clin Nutr Metab Care. 2004;7(2):137-144. http://www.ncbi.nlm.nih.gov/pubmed/15075703. Accessed September 26, 2019.
- Giltay EJ, Gooren LJ, Toorians AW, Katan MB, Zock PL. Docosahexaenoic acid concentrations are higher in women than in men because of estrogenic effects. Am J Clin Nutr. 2004;80(5):1167-1174. doi:10.1093/ajcn/80.5.1167
- Grimsgaard S, Bonaa KH, Hansen JB, Nordøy A. Highly purified eicosapentaenoic acid and docosahexaenoic acid in humans have similar triacylglycerol-lowering effects but divergent effects on serum fatty acids. Am J Clin Nutr. 1997;66(3):649-659. doi:10.1093/ajcn/66.3.649
- Phang M, Garg ML, Sinclair AJ. Inhibition of platelet aggregation by omega-3 polyunsaturated fatty acids is gender specific—Redefining platelet response to fish oils. Prostaglandins, Leukot Essent Fat Acids. 2009;81(1):35-40. doi:10.1016/j.plefa.2009.05.001
- Sublette ME, Ellis SP, Geant AL, Mann JJ. Meta-Analysis of the Effects of Eicosapentaenoic Acid (EPA) in Clinical Trials in Depression. J Clin Psychiatry. 2011;72(12):1577-1584. doi:10.4088/JCP.10m06634
- Yassine HN, Braskie MN, Mack WJ, et al. Association of Docosahexaenoic Acid Supplementation With Alzheimer Disease Stage in Apolipoprotein E ε4 Carriers. JAMA Neurol. 2017;74(3):339. doi:10.1001/jamaneurol.2016.4899
- Stoll AL, Severus WE, Freeman MP, et al. Omega 3 Fatty Acids in Bipolar Disorder. Arch Gen Psychiatry. 1999;56(5):407. doi:10.1001/archpsyc.56.5.407
- Dinan T, Siggins L, Scully P, O’Brien S, Ross P, Stanton C. Investigating the inflammatory phenotype of major depression: Focus on cytokines and polyunsaturated fatty acids. J Psychiatr Res. 2009;43(4):471-476. doi:10.1016/j.jpsychires.2008.06.003
- Minihane AM, Armah CK, Miles EA, et al. Consumption of Fish Oil Providing Amounts of Eicosapentaenoic Acid and Docosahexaenoic Acid That Can Be Obtained from the Diet Reduces Blood Pressure in Adults with Systolic Hypertension: A Retrospective Analysis. J Nutr. 2016;146(3):516-523. doi:10.3945/jn.115.220475
- Wang Q, Liang X, Wang L, et al. Effect of omega-3 fatty acids supplementation on endothelial function: A meta-analysis of randomized controlled trials. Atherosclerosis. 2012;221(2):536-543. doi:10.1016/j.atherosclerosis.2012.01.006
- Oelrich B, Dewell A, Gardner CD. Effect of fish oil supplementation on serum triglycerides, LDL cholesterol and LDL subfractions in hypertriglyceridemic adults. Nutr Metab Cardiovasc Dis. 2013;23(4):350-357. doi:10.1016/j.numecd.2011.06.003
- Hill AM, Buckley JD, Murphy KJ, Howe PR. Combining fish-oil supplements with regular aerobic exercise improves body composition and cardiovascular disease risk factors. Am J Clin Nutr. 2007;85(5):1267-1274. doi:10.1093/ajcn/85.5.1267
- Coletta JM, Bell SJ, Roman AS. Omega-3 Fatty Acids and Pregnancy. Rev Obstet Gynecol. 2010;3(4):163. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3046737/. Accessed September 26, 2019.
- Parker HM, Johnson NA, Burdon CA, Cohn JS, O’Connor HT, George J. Omega-3 supplementation and non-alcoholic fatty liver disease: A systematic review and meta-analysis. J Hepatol. 2012;56(4):944-951. doi:10.1016/j.jhep.2011.08.018
- Tosi F, Sartori F, Guarini P, Olivieri O, Martinelli N. Delta-5 and Delta-6 Desaturases: Crucial Enzymes in Polyunsaturated Fatty Acid-Related Pathways with Pleiotropic Influences in Health and Disease. In: Advances in Experimental Medicine and Biology. Vol 824. ; 2014:61-81. doi:10.1007/978-3-319-07320-0_7
- Ameur A, Enroth S, Johansson Å, et al. Genetic Adaptation of Fatty-Acid Metabolism: A Human-Specific Haplotype Increasing the Biosynthesis of Long-Chain Omega-3 and Omega-6 Fatty Acids. Am J Hum Genet. 2012;90(5):809-820. doi:10.1016/j.ajhg.2012.03.014
- Baraldi FG, Vicentini TM, Teodoro BG, et al. The combination of conjugated linoleic acid (CLA) and extra virgin olive oil increases mitochondrial and body metabolism and prevents CLA-associated insulin resistance and liver hypertrophy in C57Bl/6 mice. J Nutr Biochem. 2016;28:147-154. doi:10.1016/j.jnutbio.2015.10.008
- Dilzer A, Park Y. Implication of Conjugated Linoleic Acid (CLA) in Human Health. Crit Rev Food Sci Nutr. 2012;52(6):488-513. doi:10.1080/10408398.2010.501409
- Ziboh VA, Fletcher MP. Dose-response effects of dietary γ-linolenic acid—enriched oils on human polymorphonuclear-neutrophil biosynthesis of leukotriene B4. Am J Clin Nutr. 1992;55(1):39-45. doi:10.1093/ajcn/55.1.39
- Johnson MM, Swan DD, Surette ME, et al. Dietary Supplementation with γ-Linolenic Acid Alters Fatty Acid Content and Eicosanoid Production in Healthy Humans. J Nutr. 1997;127(8):1435-1444. doi:10.1093/jn/127.8.1435
- Barham JB, Edens MB, Fonteh AN, Johnson MM, Easter L, Chilton FH. Addition of Eicosapentaenoic Acid to γ-Linolenic Acid–Supplemented Diets Prevents Serum Arachidonic Acid Accumulation in Humans. J Nutr. 2000;130(8):1925-1931. doi:10.1093/jn/130.8.1925
- Laidlaw M, Holub BJ. Effects of supplementation with fish oil–derived n−3 fatty acids and γ-linolenic acid on circulating plasma lipids and fatty acid profiles in women. Am J Clin Nutr. 2003;77(1):37-42. doi:10.1093/ajcn/77.1.37
- Hardy ML. Herbs of special interest to women. J Am Pharm Assoc (Wash). 40(2):234-42; quiz 327-9. http://www.ncbi.nlm.nih.gov/pubmed/10730024. Accessed September 26, 2019.
- Farzaneh F, Fatehi S, Sohrabi M-R, Alizadeh K. The effect of oral evening primrose oil on menopausal hot flashes: a randomized clinical trial. Arch Gynecol Obstet. 2013;288(5):1075-1079. doi:10.1007/s00404-013-2852-6
- Ciappolino V, Mazzocchi A, Enrico P, et al. N-3 Polyunsatured Fatty Acids in Menopausal Transition: A Systematic Review of Depressive and Cognitive Disorders with Accompanying Vasomotor Symptoms. Int J Mol Sci. 2018;19(7). doi:10.3390/ijms19071849
- Keen H, Payan J, Allawi J, et al. Treatment of Diabetic Neuropathy With -Linolenic Acid. Diabetes Care. 1993;16(1):8-15. doi:10.2337/diacare.16.1.8
- Jamal GA, Carmichael H. The Effect of γ-Linolenic Acid on Human Diabetic Peripheral Neuropathy: A Double-blind Placebo-controlled Trial. Diabet Med. 1990;7(4):319-323. doi:10.1111/j.1464-5491.1990.tb01397.x
- Das UN. A defect in the activity of Δ6 and Δ5 desaturases may be a factor predisposing to the development of insulin resistance syndrome. Prostaglandins, Leukot Essent Fat Acids. 2005;72(5):343-350. doi:10.1016/j.plefa.2005.01.002
- MORSE PF, HORROBIN DF, MANKU MS, et al. Meta-analysis of placebo-controlled studies of the efficacy of Epogam in the treatment of atopic eczema. Relationship between plasma essential fatty acid changes and clinical response. Br J Dermatol. 1989;121(1):75-90. doi:10.1111/j.1365-2133.1989.tb01403.x
- Bordoni A, Biagi PL, Masi M, et al. Evening primrose oil (Efamol) in the treatment of children with atopic eczema. Drugs Exp Clin Res. 1988;14(4):291-297. http://www.ncbi.nlm.nih.gov/pubmed/3048953. Accessed October 2, 2019.
- Biagi PL, Bordoni A, Masi M, et al. A long-term study on the use of evening primrose oil (Efamol) in atopic children. Drugs Exp Clin Res. 1988;14(4):285-290. http://www.ncbi.nlm.nih.gov/pubmed/3048952. Accessed October 2, 2019.
- SCHALIN-KARRILA M, MATTILA L, JANSEN CT, UOTILA P. Evening primrose oil in the treatment of atopic eczema: effect on clinical status, plasma phospholipid fatty acids and circulating blood prostaglandins. Br J Dermatol. 1987;117(1):11-19. doi:10.1111/j.1365-2133.1987.tb04085.x
- Calder PC. Dietary modification of inflammation with lipids. Proc Nutr Soc. 2002;61(3):345-358. doi:10.1079/pns2002166
- Surette ME, Stull D, Lindemann J. The impact of a medical food containing gammalinolenic and eicosapentaenoic acids on asthma management and the quality of life of adult asthma patients. Curr Med Res Opin. 2008;24(2):559-567. doi:10.1185/030079908×273011
- Parletta N, Cooper P, Gent DN, Petkov J, O’Dea K. Effects of fish oil supplementation on learning and behaviour of children from Australian Indigenous remote community schools: A randomised controlled trial. Prostaglandins, Leukot Essent Fat Acids. 2013;89(2-3):71-79. doi:10.1016/j.plefa.2013.05.001
- Bauer I, Hughes M, Rowsell R, et al. Omega-3 supplementation improves cognition and modifies brain activation in young adults. Hum Psychopharmacol Clin Exp. 2014;29(2):133-144. doi:10.1002/hup.2379
- Riaz A, Khan RA, Ahmed SP. Assessment of anticoagulant effect of evening primrose oil. Pak J Pharm Sci. 2009;22(4):355-359. http://www.ncbi.nlm.nih.gov/pubmed/19783511. Accessed October 2, 2019.
- Ishikawa T, Fujiyama Y, Igarashi O, et al. Effects of gammalinolenic acid on plasma lipoproteins and apolipoproteins. Atherosclerosis. 1989;75(2-3):95-104. doi:10.1016/0021-9150(89)90165-2
- Guivernau M, Meza N, Barja P, Roman O. Clinical and experimental study on the long-term effect of dietary gamma-linolenic acid on plasma lipids, platelet aggregation, thromboxane formation, and prostacyclin production. Prostaglandins, Leukot Essent Fat Acids. 1994;51(5):311-316. doi:10.1016/0952-3278(94)90002-7
- Leng GC, Lee AJ, Fowkes FG, et al. Randomized controlled trial of gamma-linolenic acid and eicosapentaenoic acid in peripheral arterial disease. Clin Nutr. 1998;17(6):265-271. http://www.ncbi.nlm.nih.gov/pubmed/10205349. Accessed October 2, 2019.
- Zurier RB, Rossetti RG, Jacobson EW, et al. Gamma-linolenic acid treatment of rheumatoid arthritis. A randomized, placebo-controlled trial. Arthritis Rheum. 1996;39(11):1808-1817. doi:10.1002/art.1780391106
- Leventhal LJ. Treatment of Rheumatoid Arthritis with Gammalinolenic Acid. Ann Intern Med. 1993;119(9):867. doi:10.7326/0003-4819-119-9-199311010-00001
- Furse RK, Rossetti RG, Zurier RB. Gammalinolenic Acid, an Unsaturated Fatty Acid with Anti-Inflammatory Properties, Blocks Amplification of IL-1β Production by Human Monocytes. J Immunol. 2001;167(1):490-496. doi:10.4049/jimmunol.167.1.490
- Kast RE. Borage oil reduction of rheumatoid arthritis activity may be mediated by increased cAMP that suppresses tumor necrosis factor-alpha. Int Immunopharmacol. 2001;1(12):2197-2199. http://www.ncbi.nlm.nih.gov/pubmed/11710548. Accessed October 2, 2019.
- Sheppard JD, Singh R, McClellan AJ, et al. Long-term Supplementation With n-6 and n-3 PUFAs Improves Moderate-to-Severe Keratoconjunctivitis Sicca. Cornea. 2013;32(10):1297-1304. doi:10.1097/ICO.0b013e318299549c
Last updated on 4th August 2023 by cytoffice

This one is just too complicated for me to get my head around. Please simplify!
Thank you but way too complicated, I just need to know which product has highest DHA for my ADHD.
/hi Neil – From our Omega 3 products, our Lem-O-3 oil provides the highest level of DHA at 462.5mg per 5ml teaspoon.
Where are you found? asking from Zambia
Hello – please find out products via our website: https://www.cytoplan.co.uk/
Thank you , very helpful and informative
This seems such a complicated subject. However this article has added some clarity to the subject.
Thank you so much.
I am interested to know what is the difference between pro-inflamatory and anti-inflamatory, after reading the write-up on omega 3 + 6 as we stopped using sunflower oil and replaced it now with cooking with virgin oil – is this the right thing to do ?
Hi There – many omega 6 fatty acids, when consumed in excess and at the expense of Omega 3s, can create inflammation within our bodies – so by including the Omega 3 fatty acids EPA and GLA, either as oily fish or in supplement form, you will help to balance the ratio of fatty acids and support the reduction of inflammation. While extra virgin olive oil can have many health benefits and is good to use on salads or sautéing over a low heat, it has a low smoke point so I wouldn’t recommend it for roasting or frying – instead you should opt for oils such as avocado or coconut.
Excellent article, thank you.
Thank you